According to THE CONVERSATION
I. The Census of the Interior: Fungi Emerge from the Shadows
In the sprawling, bustling metropolis that is the human body, we’ve long focused on the loudest residents: the trillions of bacteria we call the microbiome. They are the undeniable superstars of modern health research, the headline-grabbers. Yet, a quieter, often overlooked kingdom—the fungi—has been diligently toiling in the background, a subtle but essential part of our internal ecosystem. This fungal community, known as the mycobiome, is finally stepping out of the shadows, and what researchers are finding is less a microscopic oddity and more a profound co-pilot in the journey of health.
To grasp the mycobiome’s scale, imagine a crowded city street. The bacteria are the vast, elbow-to-elbow throng, filling every corner. The fungi, by comparison, are the scattered, distinct individuals—far fewer in number, perhaps making up less than 1% of the total microbial population, particularly in the gut. But this numerical minority is deceptive. Like a handful of giants standing among millions of average people, fungi are significantly larger than bacteria, meaning they command a noticeable share of the overall biological mass. Their influence, it turns out, is measured not just in headcount, but in impact.

Source: Wikimedia Commons, CC BY-SA 4.0
II. The Dual Citizen: Candida and the Immune System’s Training
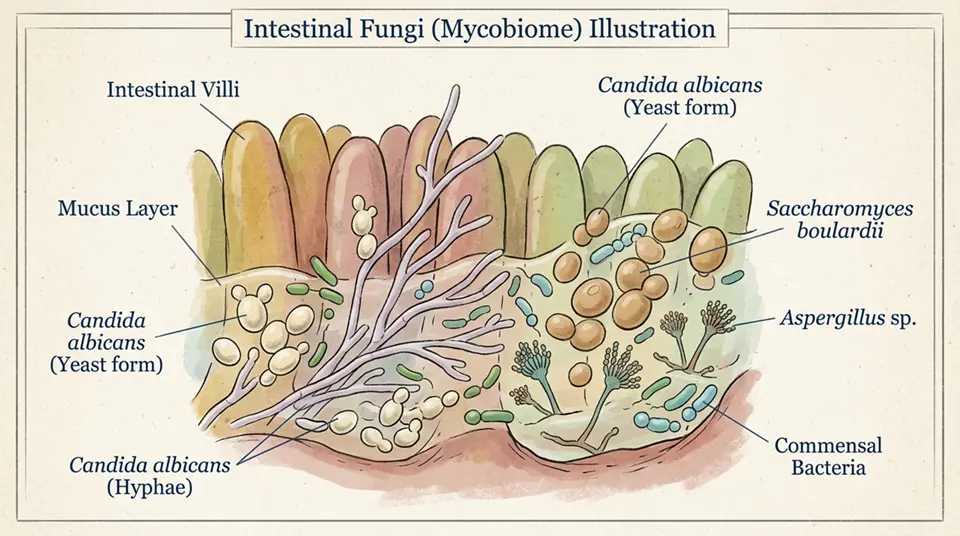
The very concept of a fungal community within us might conjure uneasy thoughts—the specter of infection, a fear rooted in moments when these organisms turn opportunistic. But to view the mycobiome solely through the lens of disease is to miss the fundamental, delicate truth: for the majority of us, for most of the time, these fungi are not invaders but long-term, established residents maintaining a biological equilibrium, a state known as homeostasis.
The most common fungal member, a type of yeast called Candida (with Candida albicans being the most frequently studied species), perfectly embodies this dual nature. In a healthy gut, it’s a benign, often beneficial presence. It participates in the intricate “housekeeping” of our intestines and, crucially, plays an unsung but vital role in training our immune system. Think of it as a sparring partner: the constant, low-level presence of these fungal antigens hones the body’s defenses, ensuring they are primed to recognize and repel actual threats. This interaction is not a clash, but a complex, cooperative dance that dictates how our body learns to tolerate friends while fighting enemies.

Source: Wikimedia Commons, Public Domain
III. The Barometer of Modern Life: Diet, Antibiotics, and Disruption
The health of this fungal landscape is a barometer, sensitive to the winds of our modern lifestyle. It is shaped from the moment we are born, influenced by everything from the mode of delivery to the earliest feeding choices. As we age, it continues to react dramatically to external factors. Diet, for instance, acts as a primary fertilizer, with certain foods favoring the growth of specific fungal species.
But perhaps the most impactful disturbance comes from the use of antibiotics. These medications, while indispensable for bacterial infections, are like a biological bulldozer: they wipe out vast numbers of the bacteria that naturally keep fungal populations in check. When the bacterial police are gone, the fungi, particularly opportunistic types like Candida, can proliferate, potentially shifting from harmless neighbors to agents of dysbiosis—an imbalance linked to inflammation and various diseases.

Source: Wikimedia Commons, CC BY-SA 4.0
IV. The Human Cost: Mycobiome Links to Gut and Brain
Recent research has begun to draw sharp lines between a disturbed mycobiome and major human health conditions. For individuals with Inflammatory Bowel Disease (IBD), such as Crohn’s disease, studies frequently reveal a distinct fungal fingerprint—specifically, an overgrowth of Candida. It’s a chicken-or-egg question: does the fungal overgrowth cause the inflammation, or does the inflamed gut create a better environment for the fungi? The most sensible interpretation, based on accumulating evidence, is a feedback loop. When a specific type of gut fungi becomes too dominant, it can produce toxins that irritate the delicate gut lining and ramp up the inflammatory activity of immune cells. It’s like a minor, localized street protest escalating into a full-blown riot, simply because the peacekeepers were absent.
Yet, the fungi’s sphere of influence isn’t limited to the digestive tract. We possess mycobiomes on our skin, in the oral cavity, and even—in low numbers—in the lungs. Some speculative but thought-provoking studies hint at a fungal role in the gut–brain axis, the critical two-way communication channel between the digestive system and the central nervous system. Early-stage research in animal models, for instance, has demonstrated that the presence of fungal cells in the brain, even at minute levels, might be linked to subtle yet measurable impairments in memory function.
V. The Path Forward: Humility and the Scientific Challenge
The challenge in studying this kingdom is profound. Fungi are notoriously difficult to culture and identify, a task made even harder by their scarcity compared to bacteria. We are, as a scientific community, still assembling the basic atlas of this inner fungal world. The technology that unlocked the secrets of the bacteriome—genomic sequencing—is now being refined to profile the mycobiome with greater accuracy, allowing us to see not just the most abundant species, but the diverse, complex web of interactions between fungi, bacteria, and the human host.
Ultimately, the revelation of the mycobiome is a call for intellectual humility and a broader lens in medicine. Health is not the simple elimination of all microbes, but the preservation of a balanced, diverse community. We must move beyond viewing fungi as mere opportunistic pathogens and begin to appreciate them as indispensable elements of our internal landscape. To restore health, we may not need to conquer this kingdom, but simply learn how to listen to its quiet, powerful voice—a voice that speaks of balance, immunity, and the profound, beautiful complexity of life within life.
References
According to THE CONVERSATION
Key Takeaways
- The human mycobiome—the community of fungi living in and on the human body—is an understudied component of the microbiome that plays significant roles in health and disease, well beyond the gut.
- Healthy humans host hundreds of fungal species across body sites including the gut, oral cavity, skin, lung, and vaginal tract, with Candida, Malassezia, Saccharomyces, and Aspergillus among the most consistently detected genera.
- The gut mycobiome interacts dynamically with bacterial microbiome members, with fungi and bacteria engaging in competitive, cooperative, and antagonistic relationships that collectively influence immune development and inflammatory disease risk.
- Disruption of the mycobiome through antifungal treatments, dietary changes, or illness contributes to dysbiosis—altered microbial community composition—that may predispose to conditions including inflammatory bowel disease, Clostridioides difficile overgrowth, and allergic disease.
- Research on the mycobiome is rapidly expanding, with sequencing approaches (ITS amplicon sequencing) enabling non-culture-based analysis of complex fungal communities—revealing fungal diversity orders of magnitude greater than previously appreciated.
Frequently Asked Questions
What is the human mycobiome and where do fungi live in the body?
The human mycobiome refers to the community of fungi that colonise various body surfaces and cavities—part of the broader human microbiome that includes bacteria, viruses, archaea, and eukaryotes. The mycobiome is present throughout the body, though fungal communities differ substantially between body sites. Body site distribution: gut mycobiome—the gastrointestinal tract hosts the most extensively studied mycobiome; predominant genera in healthy individuals typically include Candida (most abundant, particularly C. albicans and C. tropicalis), Saccharomyces (from dietary sources, including S. cerevisiae from bread and beer), Malassezia (particularly in the upper GI tract), and numerous environmental contaminants from food. Skin mycobiome—Malassezia species dominate the skin mycobiome of sebaceous areas (scalp, face, chest, back) in adults; representing up to 90–95% of all fungi detectable on healthy adult skin in these sebum-rich zones; non-sebaceous areas (feet, palms) host greater diversity including Aspergillus, Penicillium, and Rhodotorula. Oral mycobiome—the mouth harbours approximately 75–100 fungal species in healthy individuals; Candida species are most consistently detected but are not universally present; other frequently detected genera include Aspergillus, Fusarium, Rhodotorula, and Cladosporium. Pulmonary mycobiome—the lungs were formerly considered sterile but sequencing studies reveal a diverse low-biomass fungal community; Candida, Malassezia, and various environmental species are detectable; the clinical significance of the healthy lung mycobiome is actively researched. Vaginal mycobiome—dominated by Lactobacillus in the bacterial community; fungally dominated by Candida; approximately 20% of healthy women of reproductive age carry Candida without symptoms (asymptomatic colonisation).
How does the gut mycobiome interact with gut bacteria?
Gut bacteria and fungi engage in complex, dynamic interactions that collectively shape immune function, colonisation resistance to pathogens, and susceptibility to inflammatory disease—making the inter-kingdom communication within the gut microbiome a rapidly developing research focus. Key bacteria-fungi interactions in the gut: competitive exclusion and colonisation resistance: Lactobacillus species produce lactic acid, bacteriocins, and other inhibitory compounds that suppress Candida overgrowth; disruption of Lactobacillus communities (by antibiotics) frequently leads to transient Candida overgrowth—a well-documented clinical phenomenon; similarly, diverse bacterial communities outcompete fungi for epithelial attachment sites and nutrients, limiting fungal overgrowth under normal conditions. Cooperative interactions: some bacterial species create conditions that promote fungal growth—for example, Bacteroides thetaiotaomicron may provide metabolic support for Candida growth through polysaccharide breakdown products; in biofilm contexts, bacteria and fungi can form cooperative multi-kingdom biofilms with enhanced virulence and resistance to antimicrobials. Inter-kingdom signalling: Candida albicans produces farnesol, a quorum-sensing molecule that inhibits bacterial biofilm formation and influences bacterial gene expression; bacterial short-chain fatty acids (SCFAs—butyrate, propionate, acetate from fibre fermentation) influence Candida morphology switching between yeast and hyphal forms; hyphal Candida penetrates epithelial barriers; SCFA-suppressed hyphae may actually protect gut barrier function. Immune implications: the gut mycobiome drives significant immune stimulation; fungal cell wall components (β-glucans, mannans, chitins) are potent activators of innate immune receptors (Dectin-1, Dectin-2, TLR2); mycobiome training of the immune system during early life influences long-term immune calibration, possibly affecting allergy and autoimmunity risk.
What role does the mycobiome play in inflammatory bowel disease?
The mycobiome has emerged as a significant factor in inflammatory bowel disease (IBD), with consistent evidence showing dysbiotic mycobiome composition in Crohn’s disease and ulcerative colitis patients compared to healthy controls. Evidence linking the mycobiome to IBD: mycobiome dysbiosis in IBD patients: multiple studies using ITS sequencing have found altered mycobiome composition in IBD patients; Crohn’s disease patients show increased Candida tropicalis, Candida glabrata, and Saccharomyces cerevisiae; concurrent reduction in fungal diversity is observed; Malassezia restricta has been associated with Crohn’s disease severity in some studies. Anti-Saccharomyces cerevisiae antibodies (ASCA): one of the most established IBD biomarkers—ASCA antibodies (IgA and IgG) against S. cerevisiae mannan are elevated in approximately 50–60% of Crohn’s disease patients and far fewer ulcerative colitis patients; ASCA positivity predicts specific Crohn’s disease phenotypes (penetrating, fibrostenotic disease); the ASCA finding was the first major clinical evidence of a mycobiome-IBD connection, long before mycobiome sequencing studies. Mechanistic hypotheses: C. tropicalis biofilms with bacterial members (Serratia marcescens and Escherichia coli) produce more invasive biofilms than any species alone—specifically noted in IBD-associated organisms; Dectin-1 (CLEC7A) genetic variants that affect fungal pattern recognition are associated with IBD risk; antifungal activity of gut bacteria may be impaired in IBD, allowing fungal expansion. Clinical implications: antifungal therapy (fluconazole) has been explored in small IBD trials with mixed results; dietary modification affecting fungal communities (high fibre diets vs. high sugar diets with the latter promoting Candida) may influence disease activity; more rigorous clinical trials of mycobiome-targeted interventions in IBD are needed.
How is the mycobiome studied and what methods are used?
Studying the mycobiome requires specialised approaches distinct from bacterial microbiome methods, with important technical considerations that affect the validity and comparability of mycobiome studies. Key methodological approaches: Culture-based methods: traditional mycological culture on selective media (e.g., Sabouraud dextrose agar, CHROMagar Candida); advantages—identifies viable organisms, allows susceptibility testing, can detect novel species through morphological characterisation; limitations—many fastidious fungi do not culture under standard conditions; culture favours fast-growing organisms and misses slow-growing or minority species; requires several days for results. Sequencing-based (culture-independent) methods: ITS (Internal Transcribed Spacer) amplicon sequencing: the standard approach for mycobiome profiling; ITS1 or ITS2 regions of the fungal rRNA gene cluster are PCR-amplified using fungi-specific primers, then sequenced; analogous to bacterial 16S rRNA sequencing; advantages—culture-independent, detects unculturable fungi, provides diversity and relative abundance data. Challenges of mycobiome sequencing: fungal biomass in most human samples is 100–1000× lower than bacterial biomass; DNA extraction is challenging because fungal cell walls (chitin-based) are more resistant to lysis than bacterial cell walls; plant and food-derived fungal DNA in stool samples can obscure gut-resident fungi; databases for ITS sequences are less comprehensive than bacterial 16S databases; many sequences cannot be assigned beyond genus level. Shotgun metagenomics: sequences all DNA in a sample including bacteria, fungi, viruses; can identify fungi with greater specificity than ITS amplicon approaches; requires deep sequencing to detect low-biomass fungal signal; bioinformatic analysis is complex. Emerging methods: Nanopore long-read sequencing of ITS regions; digital droplet PCR for quantification of specific fungal species; culturomics (high-throughput culture under diverse conditions).
Can diet change the mycobiome and does that affect health?
Diet profoundly influences the composition and activity of the gut mycobiome, with sugar intake, fibre consumption, fermented food consumption, and alcohol intake all having documented effects on gut fungal communities—with health implications that are increasingly well characterised. Dietary factors that promote Candida overgrowth: high simple sugar diets: dietary sugars (glucose, fructose) are preferred carbon sources for Candida species; high-sugar diets consistently promote Candida overgrowth in animal models; clinical evidence in humans: diets high in added sugars are associated with higher Candida carriage rates and recurrent vulvovaginal candidiasis in some observational studies; sugar and particularly glucose supports hyphal switching in C. albicans (the invasive form). Refined carbohydrates: rapidly digestible starches (white bread, white rice) produce glucose surges in the gut lumen that preferentially feed Candida over competing organisms. Dietary factors that suppress pathogenic fungi and promote diverse mycobiome: dietary fibre: non-digestible polysaccharides fermented by gut bacteria produce short-chain fatty acids (butyrate, propionate, acetate) that suppress Candida hyphal formation; high-fibre diets are consistently associated with reduced Candida dominance and greater fungal diversity; prebiotic fibres (inulin, FOS) indirectly suppress pathogenic fungi by enhancing beneficial bacterial populations. Fermented foods: probiotic yeasts in kefir and some traditional fermented foods (Saccharomyces boulardii) have documented antifungal and barrier-protective effects; traditional fermented foods contribute to mycobiome diversity. Antifungal dietary compounds: garlic (allicin), ginger (gingerols, shogaols), coconut oil (caprylic acid, lauric acid), and various plant polyphenols have in vitro antifungal activity; clinical evidence for dietary antifungal effects sufficient to treat clinical infections is very limited, but modulating the healthy mycobiome through these dietary components may be feasible.