According to Taiwannews
Taiwan has recorded its first domestic case of valley fever (coccidioidomycosis), a rare fungal infection usually confined to arid regions in the Americas, officials confirmed this week. The case marks a significant moment in public-health surveillance and raises questions about how environmental fungal pathogens may spread beyond their traditional endemic zones.
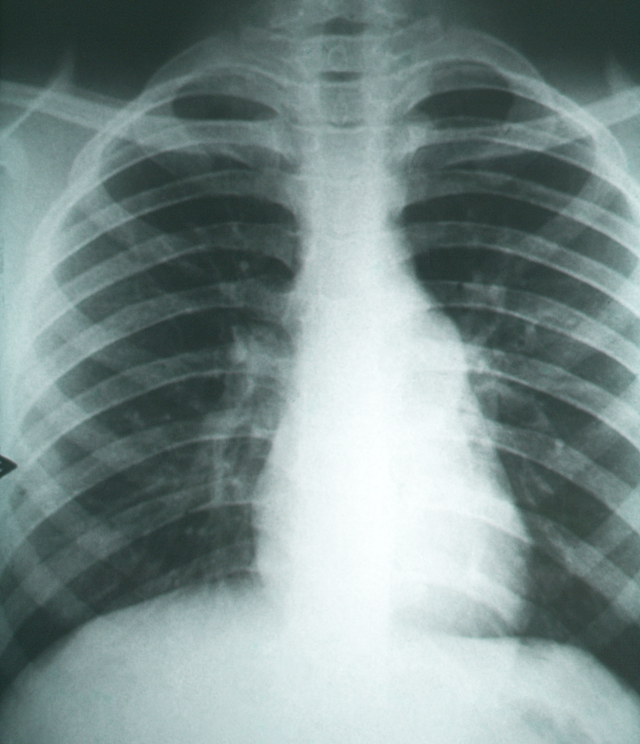
The patient, a man in his 50s from northern Taiwan, developed persistent respiratory symptoms—including shortness of breath and cough—beginning in early August. When these symptoms did not improve with initial treatment, he sought further medical care. Blood tests ultimately confirmed a diagnosis of valley fever, according to Taiwan’s Centers for Disease Control (CDC).
Valley fever is caused by inhaling spores of soil-dwelling fungi in the genus Coccidioides. Infected individuals may experience a range of symptoms, from mild, flu-like illness to severe respiratory disease. In rare cases, the infection can disseminate beyond the lungs and become life-threatening.
While Taiwan has recorded approximately 20 cases of coccidioidomycosis in the past, those were all linked to travel abroad, particularly to known endemic regions such as the southwestern United States. What distinguishes this new case is that the patient reportedly did not leave Taiwan during the disease’s incubation period, leading health authorities to classify it as a domestic case.
Source: Wikimedia Commons, CC BY-SA 3.0
What Is Valley Fever and Why It Matters
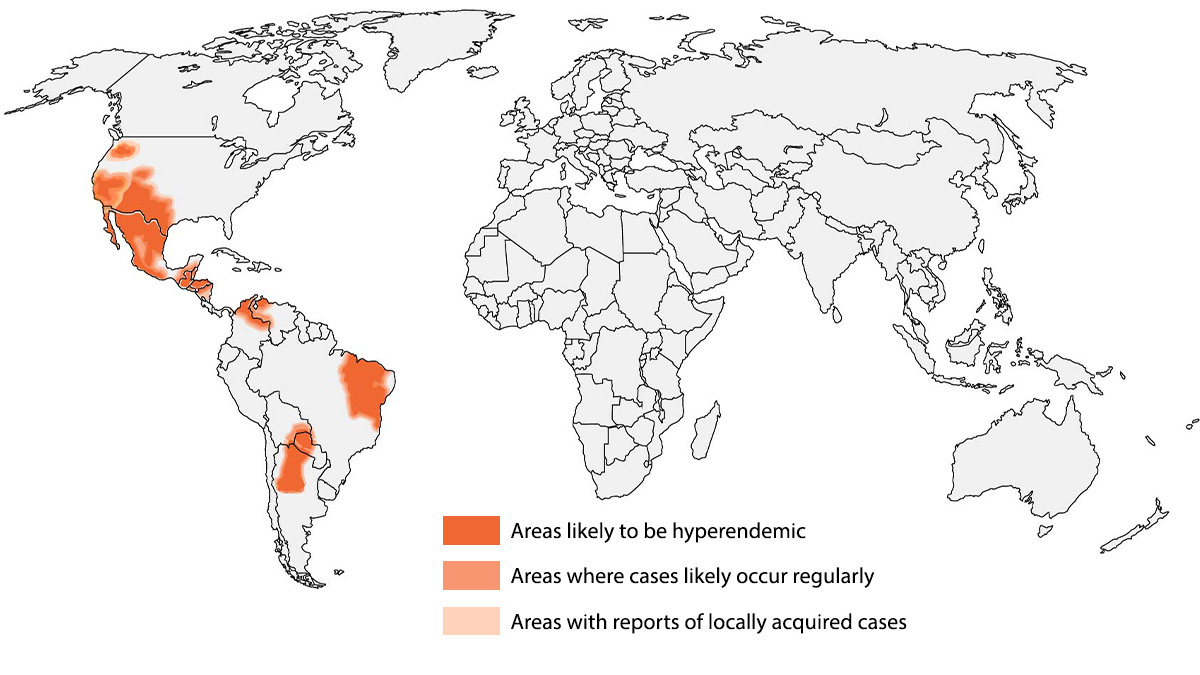
Valley fever, or coccidioidomycosis, is caused by two related fungal species: Coccidioides immitis and Coccidioides posadasii. These moulds thrive in dry, desert-like soils, especially in parts of the southwestern United States—Arizona and California’s Central Valley—the northern parts of Mexico, and regions of Central America and South America. Neither species is normally considered endemic to East Asia.
The lifecycle of Coccidioides involves a saprophytic phase in soil and an infectious phase in humans and animals. When dry soil is disturbed by wind, construction, agriculture, or human activity, microscopic fungal spores (arthroconidia) become airborne. Once inhaled, they convert to a yeast-like form that can elicit inflammatory responses in the lungs.

Source: Wikimedia Commons, CC BY-SA 4.0
Clinically, valley fever commonly presents with non-specific symptoms:
- Persistent cough
- Fever and chills
- Night sweats
- Joint and muscle pain
- Headaches
In some patients, a characteristic rash called erythema nodosum may develop. More severe disease can involve chest pain, shortness of breath, chronic pneumonia, or dissemination to skin, bone, and central nervous system—although such progression remains relatively rare.
Most infected individuals either remain asymptomatic or experience only mild illness that resolves without specific antifungal therapy. Severe disease and complications tend to occur in people with weakened immune systems, older adults, individuals with chronic conditions such as diabetes, and pregnant women.
Source: Wikimedia Commons, CC BY-SA 4.0
The Taiwan Case: Domestic Transmission or Environmental Exposure?
The domestic classification of this case is unusual because Coccidioides fungi are not known to be endemic in Taiwan. In temperate regions far from desert ecology, factors like soil type, humidity, and temperature are generally not conducive to the fungus’s environmental lifecycle.
However, health authorities speculate that the exposure may have occurred during the handling of shipping containers or other imported materials that carried dust from regions where these fungi are endemic. This mechanism—of environmental spores hitchhiking on cargo—is plausible and has been documented in other diseases where pathogens travel in soil particles attached to goods.
Because the infection is not transmitted from person to person, CDC officials emphasize that there is no evidence of community spread at this time. Instead, the focus remains on identifying environmental sources and mitigating similar exposures.
The CDC has also noted that although valley fever can be severe, the overall fatality rate remains below 1 percent, with most people recovering without notable complications.
Public-Health Implications and Surveillance
The occurrence of a domestic valley fever case in Taiwan invites reflection on broader public-health challenges relating to fungal diseases. For decades, mycotic infections have been under-recognized relative to viral and bacterial pathogens, even though environmental fungi contribute substantially to global morbidity.
In endemic areas, valley fever represents a persistent health burden, accounting for thousands of hospitalizations annually and significant healthcare costs.
This case highlights three important considerations for Taiwan and other regions beyond traditional endemic zones:
Environmental Monitoring: Fungal spores can travel long distances in dust or on imported materials, suggesting a need for environmental surveillance at ports and transport hubs.
Clinical Awareness: Healthcare providers must consider fungal diseases like coccidioidomycosis in differential diagnoses for persistent respiratory illness—even when patients have not traveled abroad.
Cross-Sector Coordination: Addressing fungal disease risk involves agricultural, environmental, transportation, and public-health sectors working together to manage soil disturbance, dust control, and pathogen monitoring.
In recent years, climate change, land use shifts, and global transport have blurred the geographic boundaries of many infectious diseases.

Source: Wikimedia Commons, CC BY-SA 3.0
Comparative Context: Imported Cases vs. Domestic Emergence
Taiwan’s report of approximately 20 valley fever cases prior to this instance were all linked to travel in endemic regions. By contrast, this case lacked any travel history abroad, suggesting local exposure.
Internationally, similar patterns have been observed when fungal diseases cross geographic boundaries due to climate shifts, human activity, or accidental transport. On a global scale, the move toward increased fungal disease recognition has prompted renewed scientific attention to how organisms like Cryptococcus, Histoplasma, and Coccidioides respond to changing ecological conditions.

Source: Wikimedia Commons, CC BY-SA 4.0
My Perspective: A Reminder of Evolving Fungal Threats
From a public-health reporting standpoint, this rare domestic valley fever case in Taiwan serves as a reminder of how fungal pathogens, long relegated to specialized medical discussions, can emerge unexpectedly. Reports of fungal disease are rising worldwide—not only in classic endemic areas but also in regions previously considered safe from such threats.
Coccidioidomycosis remains relatively rare outside its traditional endemic range, but the Taiwan case illustrates that fungal diseases can and do leap geographical boundaries, especially when human activities create opportunities for spore dispersal.
References
According to Taiwannews
Key Takeaways
- Taiwan’s confirmation of a domestically acquired Valley Fever (coccidioidomycosis) case is a significant event, suggesting that Coccidioides—the soil fungus causing this disease—may be establishing in Taiwanese soil due to changing climate or soil conditions.
- Valley Fever is caused by soil-dwelling Coccidioides immitis and C. posadasii, fungi endemic to arid and semi-arid regions of the Americas, but increasingly being detected in new geographic areas as climate change alters soil temperature and moisture regimes.
- The disease typically presents with flu-like symptoms after inhalation of Coccidioides arthroconidia (infectious spores from dry soil), but can disseminate to bones, meninges, and other organs in approximately 1% of infected individuals.
- Taiwan’s dense population, high construction activity (which disturbs soil and releases spores), and unique geological conditions make understanding whether Coccidioides has truly established there a critical public health question.
- Healthcare providers in Taiwan and other non-endemic regions must increase awareness of Valley Fever as a cause of respiratory illness, particularly in patients who have traveled to endemic areas or who live in areas with newly changing fungal ecology.
Frequently Asked Questions
What is Valley Fever and what causes it?
Valley Fever, medically termed coccidioidomycosis, is an infectious disease caused by inhaling airborne spores (arthroconidia) of two closely related soil fungi: Coccidioides immitis (found primarily in California’s San Joaquin Valley and other parts of the American Southwest) and Coccidioides posadasii (found in other parts of the Southwestern US, Mexico, and Central and South America). How Coccidioides causes disease: the fungus lives in sandy, alkaline soil in arid and semi-arid regions; during the dry season or when soil is disturbed (construction, farming, dust storms), Coccidioides releases barrel-shaped arthroconidia (infectious spores) that become airborne; inhalation of even a single arthroconidium can initiate infection; once inhaled, arthroconidia reach the lungs and transform into spherules—large, thick-walled structures filled with hundreds of endospores; spherule rupture releases endospores that each develop into new spherules, spreading infection within the lungs. Disease spectrum: most infections (approximately 60%) are asymptomatic; approximately 40% cause a respiratory illness typically resembling flu, community-acquired pneumonia, or COVID-19 (before COVID, Valley Fever was a major cause of community-acquired pneumonia misdiagnosed as bacterial pneumonia); in approximately 1–5% of infected individuals (and higher in immunocompromised), dissemination to bones, joints, skin, and meninges (meningeal coccidioidomycosis) occurs; disseminated disease is life-threatening without treatment.
Is Valley Fever spreading geographically due to climate change?
Evidence is accumulating that the endemic range of Coccidioides is expanding beyond its historically recognised boundaries, with climate change identified as a primary driver through multiple mechanisms. Historical range and current expansion evidence: traditional endemic regions—the Sonoran Desert and adjacent areas spanning parts of California, Arizona, Utah, Nevada, New Mexico, Texas, and extending through Mexico and parts of South America. Recent case distributions: Valley Fever cases have been diagnosed in patients who never travelled to traditional endemic areas—including cases in Washington State, Oregon, Montana, and other non-traditional regions; studies using environmental soil sampling have found Coccidioides DNA in soil from areas outside the historical range including parts of Central California, and more recently in soil from the Pacific Northwest. International detections: cases have been reported from non-endemic countries; the Taiwan domestic case reported in recent years is particularly notable because it suggests either locally acquired infection from Taiwanese soil, or an unrecognised environmental source. Mechanism of range expansion: Coccidioides requires specific soil conditions for persistence—warm temperatures, low moisture, alkaline pH, and specific soil microbial community conditions; as climate warms: previously temperate regions are developing warmer, drier summers resembling current Coccidioides-endemic areas; the geographic area where these conditions are met is expanding northward and to higher elevations. Modelling studies: predictive models based on Coccidioides-climate relationships project substantial range expansion under most climate change scenarios; one widely cited modelling study (Morgan et al., 2021, GeoHealth) suggested expansion of the endemic range across much of the western and central US.
Why is a domestic Valley Fever case in Taiwan significant?
Taiwan’s report of a domestically acquired coccidioidomycosis case is clinically and ecologically significant because the island is geographically far outside the traditional endemic range of Coccidioides—raising important questions about the fungus’s geographic spread. Geographic and ecological context of Taiwan: Taiwan is a subtropical island nation in the Western Pacific; its climate and soil conditions differ substantially from the arid American Southwest that is Coccidioides’ historical home; however, parts of Taiwan have warm, dry seasons and varied soil conditions; certain geological features—volcanic soils, laterite soils, and varied alkaline soil zones—might provide microhabitats suitable for Coccidioides if introduced. Why the case matters: confirms Coccidioides outside the Americas—most documented extracontinental Coccidioides cases are in travellers who visited endemic areas; a true domestic case (where the source of exposure is local soil) implies Coccidioides is present in Taiwanese environmental soil. Taiwan-specific public health implications: Taiwan has a dense population of 23+ million concentrated in relatively small land area; large-scale urban construction and infrastructure projects constantly disturb soil; typhoon events regularly disturb soil and generate dust storms—ideal conditions for amplifying Coccidioides soil-to-air dispersal if the fungus is present. Diagnostic and clinical implications: Taiwanese physicians are not trained to routinely consider Valley Fever in their differential diagnosis of respiratory illness; the condition was previously considered an imported disease in Taiwan; without clinical awareness, many cases will be misdiagnosed, delaying treatment and appropriate public health investigation.
What are the symptoms of Valley Fever and how is it diagnosed?
Valley Fever has a highly variable clinical presentation that frequently mimics more common respiratory illnesses, contributing to an average diagnostic delay of 1–2 years in endemic areas and longer in non-endemic regions. Symptom presentation: acute pulmonary coccidioidomycosis (most common form): appears 1–3 weeks after exposure; symptoms in 40% of those infected who develop any symptoms: fatigue (often severe and prolonged), cough (dry to productive), chest pain (pleuritic), fever, night sweats; approximately 5–10% of symptomatic patients develop eosinophilic pleural effusion; skin manifestations of systemic immune response: erythema nodosum (painful red nodules on shins—’Valley Fever rash’) in 5–10% of symptomatic cases, particularly women. Progressive or disseminated coccidioidomycosis: occurs in 1–5% of infected individuals; risk factors for dissemination: HIV/AIDS (major risk factor); haematological malignancy; solid organ transplant; TNF-alpha inhibitor therapy; pregnancy (second and third trimester); African American and Filipino ethnicity (genetic susceptibility factors); diabetes mellitus; sites of dissemination: lungs (worsening pneumonia, cavities), bones and joints (osteomyelitis, arthritis), skin (nodules, ulcers), meningitis (the most feared disseminated form—chronic and potentially fatal without lifelong treatment). Diagnostic tests: serology (complement fixation antibodies, immunodiffusion)—most commonly used; available commercially; becomes positive 2–6 weeks after infection. Antigen testing—detects Coccidioides antigen in urine or serum; available from specialty laboratories; useful for disseminated or immunocompromised patients who may not mount adequate antibody responses. Culture—definitive but slow (weeks) and requires BSL-3 biocontainment due to infectiousness of culture material. PCR—increasingly available at specialty laboratories.
How is Valley Fever treated and how long does treatment last?
Valley Fever treatment decisions depend on disease severity, anatomical sites of infection, immune status, and patient risk factors for dissemination. Not all cases require antifungal therapy. Treatment by disease category: mild to moderate acute pulmonary Valley Fever in immunocompetent patients: many cases resolve without antifungal treatment; active monitoring and supportive care may be appropriate; antifungal treatment is recommended for patients with prolonged symptoms (> 6 weeks), severe illness, or risk factors for dissemination; when treatment is initiated: fluconazole 400 mg/day for 3–6 months is standard first-line therapy. Severe acute pulmonary disease or diffuse infiltrates: amphotericin B initially (for more severe presentations), transitioning to azole therapy when clinical improvement occurs; usual total duration 12 months. Bone and joint coccidioidomycosis (extrapulmonary, non-meningeal): fluconazole 400–800 mg/day for minimum 12 months; often requires longer treatment based on clinical response; surgical debridement may be needed for bone involvement. Coccidioidal meningitis—the most serious form: fluconazole 400–800 mg/day is first-line; alternative: intrathecal amphotericin B (now rarely used); critical aspect: coccidioidal meningitis requires LIFELONG therapy—indefinitely—because relapse rates approach 100% when treatment is discontinued; patients must be counselled that they face life-long medication. Disseminated disease (non-meningeal): fluconazole or itraconazole 400–800 mg/day for 12 months minimum; some require life-long therapy depending on immune status and response. Posaconazole and voriconazole: used for refractory cases; may have better activity than fluconazole against specific sites of infection. Echinocandins: NOT active against Coccidioides (the cell wall target differs); not used for coccidioidomycosis.