According to THE GUARDIAN
I. The Quiet Crisis: Biodegrading Our Inner Wild
When we think of the biodiversity crisis, images of destroyed rainforests usually come to mind. However, a silent and profound ecological crisis is unfolding much closer to home—within the human body. Each human is home to its own miniature ecosystem, the human microbiome, made up of trillions of bacteria, as well as smaller communities of fungi and viruses. This is akin to how a forest relies on the biodiversity of animals, trees, and soil.
The health of these microscopic worlds is crucial. Dr. James Kinross, a reader in surgery at Imperial College London, calls the loss of this microbial biodiversity an “internal climate crisis.” He emphasizes that this depletion is directly linked to the dramatic rise in chronic conditions that plague modern society. This shifts medical thinking away from the traditional view of simply “killing all microbes” toward a more holistic, conservation-based strategy.
Source: Wikimedia Commons, CC BY-SA 4.0
II. The Drivers of Microbial Depletion
Research identifies four major ways modern Western lifestyle is eroding our vital microbial heritage:
1. Misuse of Medicines (Antibiotics)
Antibiotics are broad-spectrum weapons that destroy beneficial microbes alongside harmful ones. The overuse of these medicines acts as a biological bulldozer, damaging the microbiome’s diversity and resilience.
2. Ultra-Processed Foods
The highly refined, ultra-processed diet starves the microbes that thrive on diverse, complex plant fibers.
3. Loss of Contact with Nature (Urbanization)
Urbanization isolates people from nature, reducing time spent inhaling, touching, and ingesting beneficial microorganisms from the soil microbiome and natural environments.
4. Disconnection
We live in an increasingly disconnected way. This isolation reduces the sharing of beneficial microbes between people, which is crucial for building a diverse and resilient microbiome.
Importantly, the microbiome is not just about the gut. Skin microbiota are specialists in wound healing, and those in the vaginal microbiome keep the environment acidic to protect against invaders. Over 100 species of fungi live on the feet alone—every community is different.

Source: Wikimedia Commons, CC BY-SA 4.0
III. Reversing the Damage: A Prescription for Biodiversity
Kinross and other researchers stress that there are simple, actionable steps that shift the emphasis back to a conservation strategy for our internal ecosystem.
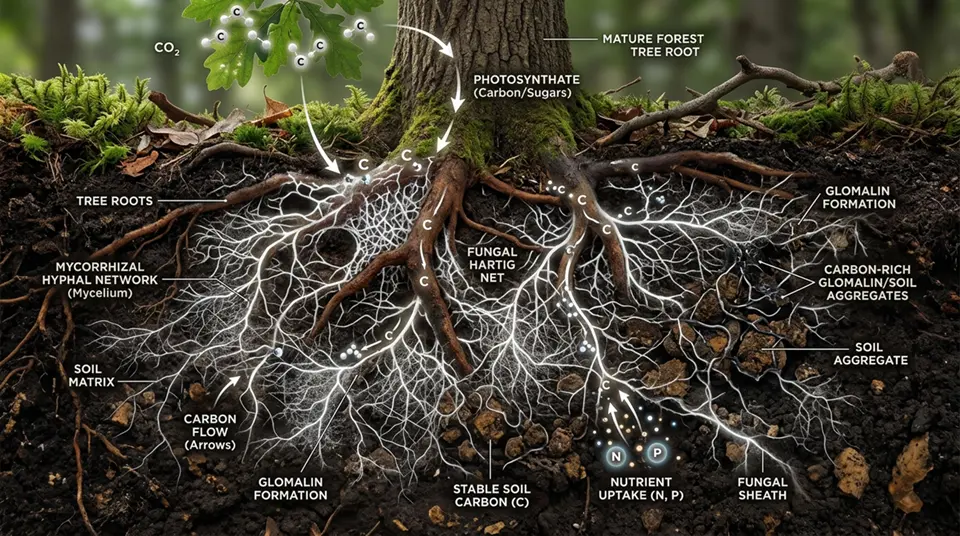
A. Reconnecting with Nature and Soil
A growing body of research links the outer layer of biodiversity (soil, water, plants) with the inner layer (the human microbiome). Exchanging microscopic bacteria, viruses, and fungi with the environment is essential.
- Rewilding Spaces:
Programs such as the Finnish biodiversity intervention are rewilding kindergarten play areas—importing forest floors into urban sites—to boost children’s exposure to beneficial microorganisms. - Bringing Nature Indoors:
A study on a green wall installed by Finnish company Naava found that within two weeks, Lactobacillus bacteria increased on employees’ skin, helping to prevent skin infections. - Gardening and Plants:
A 2020 Finnish study showed that just one month of growing plants boosted skin bacteria diversity and immune response, emphasizing the role of biodiverse soils.
B. Nurturing Social Networks
Humans are social organisms, and sharing microbiomes through contact is vital:
- Social Diversity:
Studies show that people with larger social networks have more diverse gut microbiomes.
Teenagers and elders entering care homes often experience a microbial diversity increase through new human contact. - Eating and Sharing:
Kinross recommends eating with others to share microbes, noting that every home carries its unique microbial signature. - Kissing is Beneficial:
The oral microbiome is one of the most diverse after the colon. About 80 million bacteria are exchanged in a kiss, which helps maintain microbial diversity. Kinross explicitly encourages: “Kissing is good, you should do that for your microbiome.”
IV. Conclusion: An Ecological Self-Correction
The study of the microbiome is rapidly evolving into a credible science filling lecture halls worldwide. The key message is that human health demands an ecological self-correction—a conscious move away from over-sterilization and isolation toward reconnection with nature and community.
By conserving our “inner wild,” we secure both the health and resilience of the human body.

Source: Wikimedia Commons, CC BY-SA 4.0
References
- World Health Organization (WHO). Chronic diseases overview.
- National Institutes of Health (NIH). Human Microbiome Fact Sheet.
- Nature Reviews Microbiology. Soil microbiome and biodiversity connection.
According to THE GUARDIAN
Key Takeaways
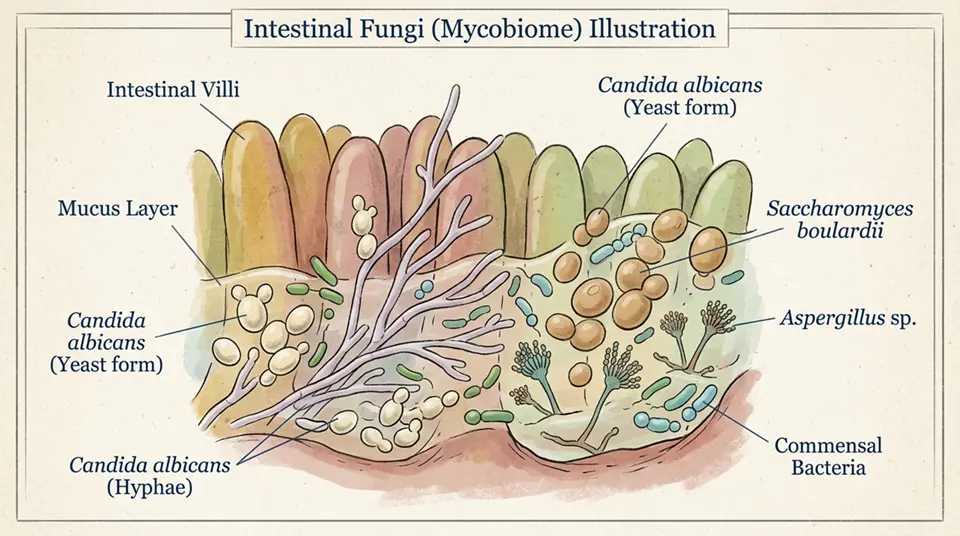
- The human gut mycobiome—the community of fungi living in the digestive tract—is now recognised as an important component of the gut microbiome alongside bacteria, with fungal communities influencing immune regulation, inflammation, and metabolic processes.
- Overuse of antibacterial antibiotics is a primary driver of gut mycobiome disruption, as broad-spectrum antibiotics kill bacterial competitors that normally suppress fungal populations, allowing fungi like Candida to overgrow.
- Modern Western dietary patterns—high in processed foods, refined sugars, and low in diverse plant fibers—reduce gut microbial diversity and alter the balance between bacterial and fungal communities in the gut.
- Early life exposure to diverse microorganisms (including environmental fungi) appears critical for appropriate immune development, with epidemiological studies linking biodiversity-poor early environments to higher rates of allergic disease and asthma.
- The ‘extinction’ of ancestral microbial lineages—organisms that co-evolved with humans over tens of thousands of years and are now being lost from Westernised populations—may have irreversible consequences for population health.
Frequently Asked Questions
What is the gut mycobiome and why does it matter?
The gut mycobiome refers to the community of fungi inhabiting the human gastrointestinal tract—a component of the broader gut microbiome that has received much less research attention than bacterial residents despite growing evidence of its importance. What’s in a typical gut mycobiome: Candida species dominate in most human gut mycobiomes, with C. tropicalis, C. albicans, and C. parapsilosis most frequently detected; Saccharomyces cerevisiae (the yeast used in baking and brewing) is commonly found; Malassezia species (primarily skin fungi) appear in gut samples; Aspergillus, Penicillium, and numerous other environmental fungi are transiently detected after dietary exposure. Numbers and relative abundance: fungi constitute a tiny fraction of gut microbial mass—bacterial cells in the gut outnumber fungal cells by approximately 1,000 to 1; however, due to the larger size of fungal cells relative to bacteria, fungal biomass may be a larger fraction than cell count would suggest. Why it matters despite low abundance: inter-kingdom interactions—gut Candida species interact extensively with bacterial residents, competing for nutrients and niches; changes in Candida abundance affect bacterial community composition and vice versa. Immune modulation—gut fungi interact with intestinal dendritic cells and macrophages through pattern recognition receptors including Dectin-1 (which recognises fungal beta-glucan); these interactions shape systemic immune tone. Clinical associations—mycobiome alterations have been documented in Crohn’s disease, ulcerative colitis, colorectal cancer, and other conditions; whether these are causative or consequential is actively studied.
How do antibiotics affect the gut fungal community?
Antibiotic-induced disruption of the gut microbiome—termed dysbiosis—affects fungi as well as bacteria, typically in ways that allow fungi to expand their populations when their bacterial competition is removed. Mechanism of antibiotic-induced fungal overgrowth: the normal gut bacterial community creates competitive inhibition of fungal populations through occupying attachment sites on the gut epithelium, competing for nutritional substrates, and producing bacteriocin and organic acid metabolites (particularly short-chain fatty acids) that inhibit fungal growth; broad-spectrum antibiotics (particularly those with activity against anaerobes, such as amoxicillin, clindamycin, and fluoroquinolones) disrupt this bacterial community; in the post-antibiotic window, Candida and other fungi face reduced competition and commonly overgrow. Clinical manifestations: oropharyngeal candidiasis (oral thrush)—common after broad-spectrum antibiotics; vaginal candidiasis—extremely common post-antibiotic complication in women; antibiotic-associated Candida intestinal overgrowth—less clearly defined clinically than oral and vaginal candidiasis, but documented in studies using culture and molecular methods. Severity spectrum: in immunocompetent adults, antibiotic-associated Candida overgrowth is typically self-limiting once the antibiotic course is completed and bacterial competitors re-establish; in hospitalised patients already immunocompromised, GI Candida overgrowth can serve as a precursor to Candida bloodstream infection if the gut barrier is also impaired (as occurs in critical illness, chemotherapy, and surgery). Recovery: gut bacterial communities typically recover within 1–4 weeks after antibiotic cessation in healthy adults, with Candida populations declining as bacteria re-establish; recovery may be slower in older adults, those with multiple antibiotic courses, or those with underlying GI disease.
What is the ‘old friends’ hypothesis and how does it relate to fungi?
The ‘old friends’ hypothesis (an updated formulation of the ‘hygiene hypothesis’) is a theoretical framework proposing that many of the chronic inflammatory conditions prominent in modern Westernised populations—allergies, asthma, inflammatory bowel disease, autoimmune conditions, certain mood disorders—result partly from the loss of exposure to organisms with which humans co-evolved over evolutionary time. Original hygiene hypothesis (Strachan, 1989): proposed that declining childhood infections due to improved sanitation and smaller family sizes was associated with increasing allergic disease; framed as ‘old infections’ being protective. Old friends reformulation (Rook, Graham, 2003): critically refined the hypothesis to focus not on infections per se, but on ‘old friends’—organisms that humans were continuously exposed to throughout evolutionary history and that educated the immune system; these include helminths (parasitic worms), commensal microorganisms from soil and environmental exposure, and members of the normal microbiome that have been with humans throughout evolutionary history. Role of fungi in the ‘old friends’ framework: environmental fungi—spores of soil fungi (Aspergillus, Penicillium, Cladosporium) and decaying plant fungi were ever-present in human environments for most of evolutionary history; modern urban lifestyles have dramatically reduced outdoor environmental fungal exposure (particularly in urban environments); some researchers propose that this reduced exposure affects immunological education similarly to reduced bacterial exposure. Loss of ancestral commensal fungi: some commensal gut fungal lineages appear less prevalent in Westernised compared to traditional populations in early studies; whether this represents ‘extinction’ of ancestral commensal fungi is actively investigated.
Are some modern health problems linked to losing our ancestral microbiome?
A growing body of epidemiological and microbiome research supports associations between reduced microbial diversity in modern Westernised populations and rising rates of several chronic diseases, though establishing causation versus correlation remains challenging. Diseases associated with microbiome depletion: allergic diseases—the most robustly evidenced associations link reduced early-life microbial diversity with higher rates of atopic dermatitis, allergic rhinitis, food allergy, and asthma; farm children have lower rates of allergic disease than non-farm children, associated with higher environmental microbial diversity. Inflammatory bowel disease—IBD (Crohn’s disease, ulcerative colitis) rates have risen dramatically in industrialised countries; gut microbiome diversity is reduced in IBD; animal model studies demonstrate causation for specific microbial depletions in IBD development; Faecalibacterium prausnitzii depletion is a consistent finding in Crohn’s disease. Type 1 diabetes—rising T1D rates in Westernised countries with microbiome alterations proposed as contributing factors; T1D risk associates with specific early-life microbiome patterns. Obesity and metabolic syndrome—gut microbiome composition affects energy extraction from food and metabolic signalling; certain bacterial lineages are depleted in obese individuals; germ-free mice colonised with obese-mouse microbiota gain more weight than those colonised with lean-mouse microbiota. Fungal component: gut mycobiome diversity is reduced in patients with IBD, particularly Crohn’s disease; Candida tropicalis has been specifically implicated in Crohn’s disease pathogenesis through biofilm formation and intestinal barrier disruption; whether restoring lost fungal lineages would improve these conditions is experimentally unexplored.
Can we restore or protect our microbiome diversity?
Microbiome restoration and protection is an active research and clinical frontier, with several evidence-based approaches already available and more experimental interventions under investigation. Dietary approaches with established evidence: dietary fibre diversity—fibre fermentation by gut bacteria produces short-chain fatty acids (butyrate, propionate, acetate) that feed colonocytes, regulate immune responses, and support microbial diversity; consuming 30+ different plant foods per week (vegetables, fruits, legumes, grains, nuts, seeds) has been associated with greater gut microbial diversity in large cohort studies; fermented foods—regular consumption of fermented dairy (yoghurt, kefir), fermented vegetables (kimchi, sauerkraut), and fermented soy products (miso, tempeh, natto) introduces live microorganisms that can transiently colonise the gut and may support resident microbial diversity; a randomised controlled trial (Wastyk et al., 2021, Cell) found that a high-fermented-food diet increased gut microbial diversity and reduced inflammatory markers more than a high-fibre diet alone; reduced antibiotic use—minimising unnecessary antibiotic prescriptions is the most direct way to prevent antibiotic-associated microbiome disruption; patients should discuss alternatives with their physician when antibiotics are being considered for self-limiting infections. Probiotic use: probiotics (defined preparations of live microorganisms) show modest benefits for specific conditions; Lactobacillus rhamnosus GG has the strongest evidence for preventing antibiotic-associated diarrhoea; Saccharomyces boulardii (technically a yeast) prevents antibiotic-associated diarrhoea and Clostridioides difficile infection; general probiotic supplementation for ‘microbiome restoration’ lacks strong evidence. Faecal microbiota transplantation (FMT): the most effective microbiome restoration intervention; FDA-approved for recurrent C. difficile infection; under investigation for IBD, metabolic disease, and other conditions.