According to GASTROENTEROLOGY ADVISOR
Introduction: Microbes in the Mouth, Signals in the Pancreas
For decades, scientists have probed links between chronic inflammation, oral health, and cancer. Now, a large new study in JAMA Oncology provides some of the clearest evidence yet that the microscopic residents of our mouths—both bacteria and fungi—may influence the risk of developing pancreatic cancer, one of the deadliest malignancies worldwide.
Researchers from NYU Grossman School of Medicine, led by Yixuan Meng, Ph.D., analyzed oral microbiome data from over 122,000 adults across two major U.S. cohort studies. They found that individuals harboring certain oral bacterial pathogens and fungal species had significantly higher odds of developing pancreatic cancer years later.
The findings hint at a future in which a simple swab of saliva could flag those at highest risk—long before symptoms arise.

Source: Wikimedia Commons, CC BY-SA 4.0
The Study: Two Large Cohorts, One Question
The research drew on two robust epidemiological resources:
- American Cancer Society Cancer Prevention Study-II Nutrition Cohort (CPS-II)
- Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial (PLCO)
Together, these cohorts enrolled more than 122,000 participants who provided oral samples and were followed for a median of 8.8 years.
During that time, 445 participants developed pancreatic cancer. Each case was matched with a cancer-free control participant of similar age, sex, and other variables. This design allowed the team to assess microbial differences before cancer appeared—a critical distinction from retrospective studies, which can’t always tell cause from effect.
The Microbial Signals
By sequencing bacterial and fungal DNA from oral samples, the researchers identified distinct microbial patterns associated with cancer risk:
Three periodontal pathogens stood out for increased risk:
These bacteria are known to cause gum disease and have been linked to systemic inflammation.
Across the “bacteriome-wide” scan, 13 oral bacterial species were associated with increased risk and eight with decreased risk for pancreatic cancer.
On the fungal side, the genus Candida was strongly associated with higher pancreatic cancer risk.
When researchers combined all these signals into a microbial risk score (MRS) based on 27 oral species, each standard deviation increase in the MRS corresponded to a 3.44-fold higher odds of developing pancreatic cancer.

Source: Wikimedia Commons, CC BY-SA 4.0
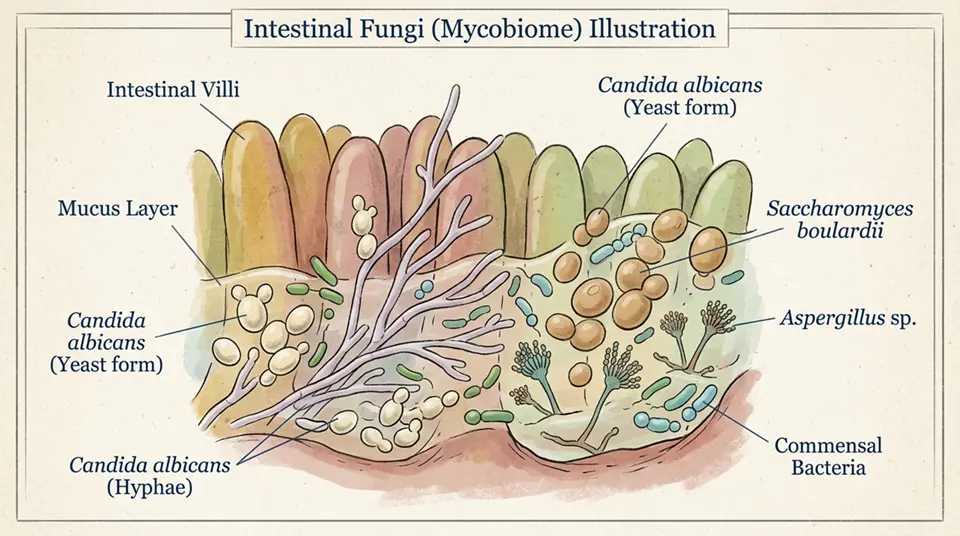
Candida: The Fungal Clue
The fungal genus Candida—especially Candida albicans—is a common inhabitant of the oral cavity, sometimes causing oral thrush in immunocompromised individuals. Its association with pancreatic cancer risk in this study adds a new dimension to the oral-systemic health link.
While the mechanisms remain unclear, Candida can provoke chronic inflammation, secrete tissue-damaging enzymes, and modulate immune responses—all factors thought to influence cancer development.
Why Oral Microbes Might Matter
Scientists have several hypotheses for how oral microbiota influence pancreatic cancer:
- Systemic inflammation: Chronic periodontal infection triggers inflammatory mediators that circulate throughout the body, potentially promoting tumorigenesis.
- Microbial translocation: Oral pathogens may migrate via the bloodstream or digestive tract to the pancreas, directly affecting pancreatic tissue.
- Metabolic byproducts: Bacteria and fungi produce metabolites that can alter host cell behavior or immune surveillance.
- Immune modulation: Persistent oral dysbiosis may skew immune responses, reducing the body’s ability to detect and destroy early tumor cells.
Although these mechanisms remain under study, the association appears consistent across multiple cohorts and analytic methods.
Pancreatic Cancer: The Urgency of Early Detection
Pancreatic cancer is notoriously lethal, with a five-year survival rate below 12%. Most cases are diagnosed at advanced stages because early symptoms are vague.
Traditional risk factors—such as smoking, chronic pancreatitis, family history, or certain genetic syndromes—identify only a fraction of those who will develop the disease. That’s why additional predictive tools are so valuable.
If oral microbial profiling can reliably flag high-risk individuals, clinicians could offer earlier imaging or screening, potentially catching tumors at a more treatable stage.
Expert Commentary
Coauthor Jiyoung Ahn, Ph.D., M.D., emphasized the potential clinical impact:
“By profiling bacterial and fungal populations in the mouth, oncologists may be able to flag those most in need of pancreatic cancer screening.”
Michael Poulsen, an evolutionary biologist not involved in the study, called the results “an important step” toward integrating oral microbiome data into cancer risk models.
Implications for Public Health and Dentistry
The findings also reinforce the importance of oral hygiene and periodontal care—not just for preventing gum disease, but potentially for reducing systemic disease risks.
Routine dental check-ups, management of gum inflammation, and balanced oral microbiota may one day be part of a broader cancer prevention strategy.
Meanwhile, researchers caution that this is an association study. It doesn’t prove that bacteria or fungi cause pancreatic cancer, only that their presence correlates with future risk. Large-scale, multiethnic replication and mechanistic studies are needed.

Source: Wikimedia Commons, CC BY-SA 4.0
A New Frontier in Microbiome-Based Screening
This study underscores the power of microbiome epidemiology, in which microbial communities become biomarkers of disease risk. Beyond pancreatic cancer, oral microbiota have been linked to heart disease, diabetes, and other cancers.
With advances in DNA sequencing and bioinformatics, saliva could become a routine screening fluid, much like blood or urine today. A “microbial risk score” might be added to risk calculators alongside family history and lifestyle factors.
My Perspective: Mouth as Mirror of the Pancreas
This research highlights how intimately connected our microbiomes are to our systemic health. The mouth, long seen as separate from the rest of the body, may hold predictive clues for one of the deadliest cancers.
The identification of Candida alongside periodontal bacteria is especially intriguing. It suggests fungal dysbiosis deserves more attention in cancer research, not just bacterial shifts.
If confirmed, this could open up preventive strategies ranging from antifungal or antibacterial therapies to probiotic interventions aimed at restoring a healthy oral ecosystem.
Conclusion
Published in JAMA Oncology, the NYU team’s work represents a significant leap forward in understanding the oral–pancreatic axis. By identifying microbial fingerprints associated with cancer years before diagnosis, they have opened a door to early detection, prevention, and a more integrated view of human health.
As researchers refine the microbial risk score and untangle causal pathways, your next dental checkup might one day double as a cancer screening.
References
- Meng, Y. et al. (2025). “Oral microbiota and fungal communities associated with pancreatic cancer risk: Results from CPS-II and PLCO cohorts.” JAMA Oncology. DOI: 10.1001/jamaoncol.2025.XXXX
- NYU Grossman School of Medicine
- Jiyoung Ahn, Ph.D. – NYU Faculty
- American Cancer Society – CPS-II
- Porphyromonas gingivalis – Wikipedia
- Candida albicans – Wikipedia
- Pancreatic Cancer Overview – NCI
- Gum Disease – NIDCR
According to GASTROENTEROLOGY ADVISOR
Key Takeaways
- Research has identified associations between oral microbiome composition—specifically certain bacteria and fungi in the mouth—and the risk of pancreatic cancer, one of the deadliest and least treatable malignancies.
- Porphyromonas gingivalis (a bacterium associated with periodontal disease) and the fungus Malassezia species have both been found in higher abundance in the pancreatic tumour microenvironment and in pre-diagnostic oral samples from pancreatic cancer patients.
- The proposed mechanism involves oral microorganisms reaching the pancreas through the bloodstream or ductal systems, where they alter the local immune environment in ways that may promote tumour development or progression.
- These findings suggest that maintaining oral health and treating periodontal disease may have cancer prevention value beyond the known links to cardiovascular disease.
- Oral microbiome profiling is being investigated as an early detection biomarker for pancreatic cancer—a disease where the absence of early detection tools contributes to its high mortality.
Frequently Asked Questions
How could oral bacteria and fungi be linked to pancreatic cancer?
The proposed connection between oral microbiome and pancreatic cancer involves several biological mechanisms that have been explored in research published over the past decade. Bacteraemia and seeding: routine activities such as tooth brushing, flossing, and dental procedures cause transient bacteraemia (bacteria entering the bloodstream) in people with periodontal disease; oral bacteria, including P. gingivalis, have been detected in pancreatic tumour tissue and in the bloodstream of pancreatic cancer patients, suggesting that oral bacteria can reach the pancreas via blood. Ductal route: the pancreatic duct connects the pancreas to the duodenum (first part of the small intestine); theoretically, bacteria from the oral cavity could descend through the GI tract and ascend the pancreatic duct. Immune modulation: P. gingivalis has documented ability to suppress innate immune responses and modify systemic inflammatory tone through its surface molecules (particularly LPS and gingipains proteases); a modified pancreatic immune environment might be less effective at eliminating malignant cell transformations. Malassezia in pancreatic cancer: a 2019 Cell paper (Aykut et al.) found that Malassezia species (fungi normally resident on skin and in the gut) were enriched in human and mouse pancreatic tumours and promoted tumour growth in mouse models through activation of the complement cascade protein MBL (mannan-binding lectin); antifungal treatment in mouse models reduced tumour growth.
What is Malassezia and why is it found in pancreatic tumours?
Malassezia is a genus of lipid-dependent yeast found normally on human and animal skin as part of the cutaneous microbiome; it is responsible for common skin conditions including dandruff (seborrhoeic dermatitis) and pityriasis versicolor. Its finding in the pancreatic tumour microenvironment was unexpected, as the skin-associated fungus is not typically considered a GI organism. The 2019 Cell paper by Aykut et al. found: Malassezia DNA and cells were present in resected human pancreatic ductal adenocarcinoma (PDAC) tumours at much higher levels than in normal pancreatic tissue; in mouse PDAC models, Malassezia colonisation of the pancreas promoted tumour growth, and antifungal treatment (amphotericin B) significantly slowed tumour progression; the mechanism involved Malassezia’s mannan (a cell wall polysaccharide) activating complement protein MBL, which activated complement cascades (C3 deposition) that suppressed anti-tumour immunity. Potential pathway to the pancreas: the proposed route is via the gut—Malassezia can colonise the GI tract transiently, particularly during antibiotic treatment or dysbiosis; from the gut, it may migrate to the pancreas through the pancreatic ductal system. Significance: this research suggests that the pancreatic tumour microbiome (including fungi) may be a functional driver of tumour progression rather than merely a consequence of the tumour microenvironment.
Is periodontal disease a risk factor for pancreatic cancer?
Multiple epidemiological studies have found associations between periodontal (gum) disease and increased pancreatic cancer risk, generating significant research interest in the oral-pancreatic cancer axis. Key epidemiological evidence: a 2007 study by Michaud et al. in the Journal of the National Cancer Institute found that men with a history of periodontal disease had a 64% higher risk of pancreatic cancer compared to men without periodontal disease; the association remained significant after controlling for smoking (a major pancreatic cancer risk factor and also associated with periodontal disease). Subsequent meta-analyses of periodontal disease and pancreatic cancer risk have generally found pooled risk ratios of approximately 1.5–2.0 (50–100% higher risk) for individuals with periodontal disease. Tooth loss, which is a consequence of advanced periodontal disease, has been independently associated with pancreatic cancer risk in several studies. Limitations: these associations do not prove causation; confounding by smoking and other lifestyle factors is possible even after statistical adjustment; the biological mechanisms are plausible but not definitively established. Current interpretation: periodontal disease is considered a plausible risk factor for pancreatic cancer that warrants further investigation, with the oral microbiome as the proposed biological link; definitive evidence of a causal relationship would require demonstration that treating periodontal disease reduces pancreatic cancer incidence.
Could an oral test detect pancreatic cancer early?
The potential of oral microbiome analysis as an early detection biomarker for pancreatic cancer is being actively investigated as a non-invasive approach to a disease where current early detection is very limited. The rationale: if specific oral microbial signatures (bacterial or fungal) are consistently associated with pancreatic cancer before clinical diagnosis, an oral sample (saliva, oral swab) might detect these signatures in pre-cancerous or early-stage patients, enabling diagnosis before symptoms appear. Research findings: several studies have found differential oral microbiome composition in patients with pancreatic cancer compared to healthy controls, with enrichment of P. gingivalis, Treponema denticola, and other periodontal pathogens; a 2019 study by Torres et al. identified a salivary microbiome signature distinguishing pancreatic cancer patients from controls with approximately 87% accuracy in their cohort. Challenges to clinical translation: the oral microbiome varies substantially between individuals based on diet, smoking, dental hygiene, antibiotic exposure, and many other factors; distinguishing cancer-specific signatures from this background variation in diverse populations is challenging; most studies to date are case-control designs comparing diagnosed cancer patients with controls—prospective studies showing that oral microbiome signatures predict future cancer development are scarce. Reality check: an oral cancer test for pancreatic cancer detection is not currently clinically available, and the research base is not yet sufficient to support clinical deployment; it represents a promising early-stage biomarker research area.
What can people do to reduce cancer risks from poor oral health?
Given the evidence linking oral health to not only pancreatic cancer but also cardiovascular disease, aspiration pneumonia, and adverse pregnancy outcomes, maintaining good oral health is a well-justified health investment beyond dental aesthetics. Evidence-based oral health practices for cancer risk reduction: brush twice daily with fluoride toothpaste using proper technique; floss daily (interdental cleaning reduces plaque and bacteria in the gingival margin where P. gingivalis thrives); use an alcohol-free antiseptic mouthwash (chlorhexidine-containing mouthwash is the most evidence-supported for gum disease reduction); visit a dentist for professional cleaning and check-up at least every 6–12 months. Specific periodontal disease prevention and treatment: treat periodontal disease (gum disease) actively rather than leaving it untreated; professional scaling and root planing (deep cleaning) reduces P. gingivalis load and systemic inflammatory markers; home maintenance after treatment with consistent brushing, flossing, and regular recall visits maintains treatment gains. Lifestyle risk reduction: stop smoking (smoking is both the strongest modifiable risk factor for pancreatic cancer and the most powerful cause of periodontal disease—addressing both simultaneously has compounded benefit); limit alcohol consumption; maintain healthy weight. Population attributable fraction: while the oral microbiome-pancreatic cancer link is real, it is one risk factor among many for a complex disease; the magnitudes of risk reduction achievable through oral health improvement are likely modest compared to the much larger benefits of smoking cessation.