
Could the air inside your home be affecting your mood? A groundbreaking new study says yes—especially if you’re older and living with mold. In rural China, where many elderly residents still rely on traditional cooking fuels and live in aging homes, scientists have uncovered a hidden link between indoor air quality and mental health. The culprit? Common household mold.

Researchers analyzed data from over 9,200 older adults as part of the Chinese Longitudinal Healthy Longevity Survey. They found that seniors exposed to indoor mold were more than twice as likely to suffer from depression or anxiety compared to those in mold-free homes. This association held strong even when controlling for income, education, and other social factors.
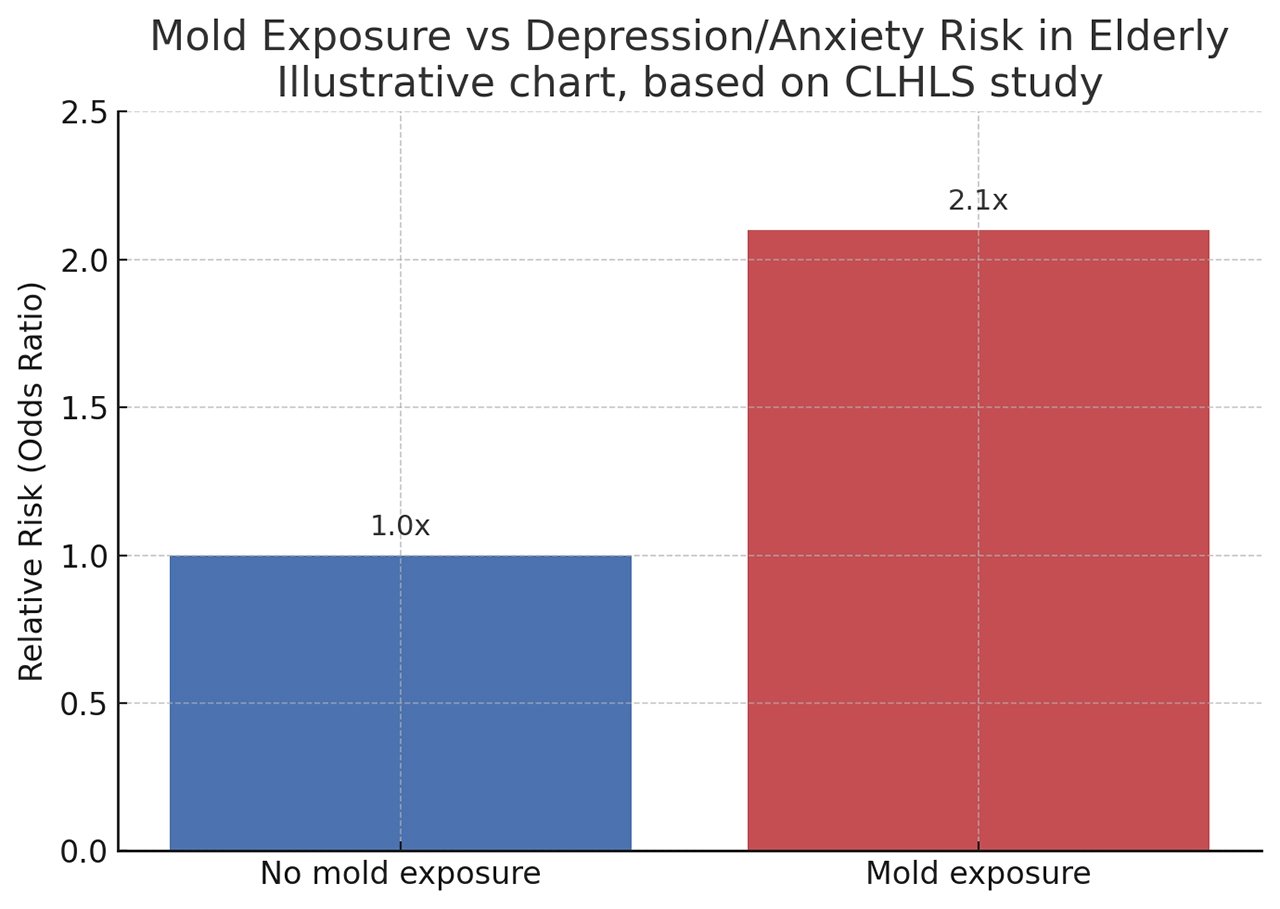
No mold exposure = 1.0x, Mold exposure ≈ 2.1x
But the picture gets more complex. The study also examined solid fuel use, like coal and wood-burning stoves. These are still widely used in rural Chinese households and were found to independently increase risks of anxiety and depression. Interestingly, in homes that used solid fuels, the anxiety risk from mold exposure appeared slightly lower—though researchers aren’t yet sure why.

What does this mean? It suggests a dual environmental burden for many older adults: poor ventilation and invisible fungal growth may be quietly undermining both physical and emotional wellbeing. Mold is no longer just an aesthetic issue or allergen—it may be a mental health hazard, especially for vulnerable populations.
How exactly mold affects the brain remains under investigation. Scientists hypothesize that inhaled fungal spores or mycotoxins may trigger inflammatory pathways, alter stress hormones, or lead to chronic stress by degrading the comfort and cleanliness of the home environment. These effects could disrupt emotional stability, particularly in older adults who spend more time indoors and may already face isolation.
So what can be done? The researchers urge a shift in public health focus. Indoor mold remediation and a transition to cleaner cooking fuels should be part of aging and housing policy, particularly in humid or poorly ventilated regions. Mental health screening could also include assessments of home environments, especially for elderly individuals reporting mood changes.
With climate change expected to increase indoor dampness globally, these findings are a timely call to action. Clean air isn’t just about lungs—it’s about emotional resilience, cognitive health, and dignity in aging.
Public policy, housing design, and community care must all take this message to heart. Because protecting our elders begins with ensuring they have safe, clean, and dry places to call home.

References
- WHO. Depression Fact Sheet. WHO.int
- WHO. Mental Disorders. WHO.int
- WHO. Mycotoxins Fact Sheet. WHO.int
- WHO. Ageing and Health. WHO.int
- PubMed. Indoor air, mold and depression in elderly. PubMed
- Chinese Longitudinal Healthy Longevity Survey. Dataset
- IPCC. Climate Change Reports. IPCC.ch
- Wikipedia. Mold, Fungal spores, Rural society in China
Key Takeaways
- Emerging research links indoor mold exposure with mental health outcomes beyond physical respiratory effects, including increased rates of depression, anxiety, and cognitive decline—particularly in elderly populations.
- The elderly are disproportionately vulnerable to mold-related health effects because they spend more time indoors, have reduced immune function, and are more likely to live in older housing with moisture problems.
- Mycotoxins from indoor molds can cross the blood-brain barrier and have been demonstrated to produce neuroinflammatory effects that affect mood regulation and cognitive function in animal models.
- The ‘sick building’ effect—non-specific symptoms including fatigue, difficulty concentrating, headaches, and low mood that improve when leaving the building—may be partly mediated by mold mycotoxin exposure.
- Improving indoor air quality in social housing for elderly residents through mold remediation and ventilation upgrades is associated with significant mental health improvements in follow-up studies.
Frequently Asked Questions
Can indoor mold exposure affect mental health and brain function?
Evidence for indoor mold exposure affecting mental health is growing and plausible mechanistically, though establishing definitive causal relationships is methodologically challenging in human studies. Evidence from human studies: epidemiological surveys consistently find associations between living in homes with visible mold or moisture problems and higher rates of depression, anxiety, and cognitive complaints; a 2007 study by Brown University found that people living in homes with mold had 40–50% higher odds of depression after controlling for confounders. The ‘World Health Organization Guidelines for Indoor Air Quality’ (2009) chapter on dampness and mould acknowledges the psychological as well as physical health effects of mold-affected housing. Mechanisms: several biologically plausible mechanisms connect mold exposure to mental health effects; mycotoxins crossing the blood-brain barrier with neuroinflammatory effects; direct neurological effects of inhaled volatile organic compounds (MVOCs) produced by mold; psychosocial stress from living in deteriorating housing; and chronic inflammatory responses from mold exposure that increase cytokine levels affecting brain function (as in the cytokine-depression hypothesis more broadly).
Why are elderly people especially vulnerable to mold-related health effects?
Multiple age-related factors converge to make elderly individuals particularly susceptible to health consequences of indoor mold exposure. Altered immune function: immunosenescence (age-related decline in immune system function) reduces the capacity to contain fungal colonisation of the respiratory tract and reduces the clearance of mycotoxins and inflammatory mediators; elderly individuals experience more severe respiratory and systemic consequences of equivalent mold exposure compared to healthy younger adults. Time indoors: elderly individuals typically spend 20–23 hours per day indoors, compared to 15–18 hours for working-age adults; higher indoor time means higher total dose from any given level of indoor mold contamination. Residential stability: elderly individuals are more likely to have lived in the same home for decades—both increasing cumulative exposure duration and meaning that mold problems that developed over years have not prompted them to move. Comorbidities: pre-existing respiratory conditions (COPD, asthma, chronic rhinitis), cardiovascular disease, and diabetes—all more prevalent in elderly populations—increase vulnerability to respiratory and systemic effects of mold exposure. Cognitive status: cognitive decline in elderly individuals can impair detection of building problems and reduce help-seeking for remediation.
What is the relationship between mold and depression?
The association between mold exposure and depression has been documented in multiple studies and operates through several potential pathways. Epidemiological evidence: the 2007 Brown University study by Brown & Bhagwat found that individuals living in mold-affected housing had approximately 50% higher odds of depression compared to those in mold-free housing after adjusting for socioeconomic factors; subsequent studies in European housing have replicated associations between dampness, mold, and depression. Psychosocial pathway: living in deteriorating, mold-damaged housing is stressful, stigmatising, and demoralising; the loss of sense of home safety and control over the living environment contributes to depressive cognitions independent of biological mechanisms; remediation studies show that improving housing conditions produces mental health benefits even when controlling for biological mold exposure changes. Inflammatory pathway: chronic low-grade inflammation from mold-related immune activation increases circulating cytokines (IL-6, TNF-α, IL-1β) that are consistently associated with depressive symptoms; the inflammatory theory of depression (Dantzer et al., 2008) provides a mechanistic framework for understanding how immune activation from any persistent pathogen or allergen exposure could contribute to depression. Mycotoxin pathway: mycotoxins that reach the CNS produce neuroinflammatory effects and may affect monoamine neurotransmitter systems; this is less well-established in humans but supported by animal model data.
Can improving home air quality improve mental health in elderly residents?
Evidence from intervention studies supports that improving indoor air quality (including mold remediation) in homes occupied by elderly residents produces mental health benefits alongside physical health improvements. The most relevant evidence base: the UK’s Warm Homes initiative and subsequent evaluations found that energy efficiency improvements (which often included improved ventilation and damp/mold control) in social housing for elderly residents produced measurable mental health benefits, including reduced depression symptom scores and improved subjective wellbeing. New Zealand studies of healthy homes standards interventions—including mold remediation and heating improvements—found significant improvements in mental health survey scores in elderly occupants compared to control households. Asthma and respiratory studies: interventions that reduce asthma triggers (including mold) in homes show improvements in mental health outcomes in occupants with asthma; this is partly mediated through reduced disease burden but the housing condition improvements themselves appear to have independent mental health effects. Practical implications: mold remediation in housing for elderly residents should be viewed as a healthcare-relevant intervention, not merely a building maintenance issue; the mental health co-benefits of remediation are relevant to cost-effectiveness assessments and healthcare-housing partnership programmes.
What specific air quality improvements most benefit elderly mental health?
Research and public health practice have identified specific indoor air quality improvements with documented mental health co-benefits for elderly occupants. Mold and dampness remediation: addressing visible mold and moisture sources is consistently the most impactful single intervention in dampness-related housing. Temperature improvements: cold indoor temperatures (below 18°C in habitable rooms) are independently associated with both physical and mental health harms; heating and insulation improvements that maintain minimum indoor temperatures benefit both respiratory and psychological health. Particulate matter reduction: HEPA filtration reducing indoor PM2.5 from both indoor sources and outdoor infiltration has been shown to reduce inflammatory markers; emerging data suggests this translates to mental health benefits. Noise reduction: though not mold-specific, addressing traffic noise infiltration—which disrupts sleep and is independently associated with depression—through improved window sealing may compound the mental health benefit of other air quality improvements. CO and gas exposure reduction: replacing gas cooking and heating with electric alternatives reduces indoor nitrogen dioxide and, where combustion appliances are poorly maintained, CO; both pollutants have direct neurological and mental health effects. Integration with social needs: home assessment programmes that simultaneously address indoor environmental quality and social isolation (through social worker engagement) achieve better mental health outcomes than purely technical interventions.







