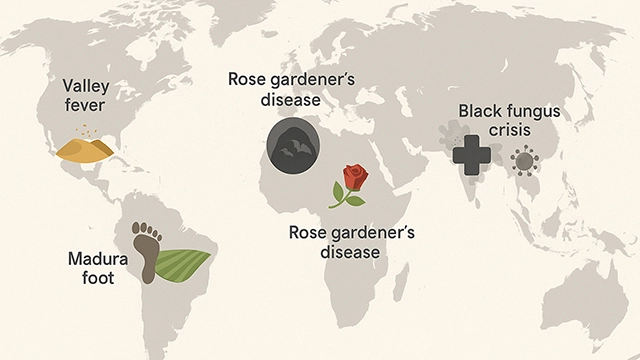
When people think of mold, most imagine bread turning green in the kitchen, black spots in the bathroom, or the musty smell in a wardrobe during the rainy season. These “small household troubles” seem unrelated to disease risk. But on a global scale, fungi are not only found in damp corners of the home—they can also cause distinctive diseases in specific regions and seasons. Some of these diseases even have catchy names that reflect the local environment, becoming part of everyday conversation. Let us open a “global fungal endemic disease map” and see how these illnesses connect to daily life.
Valley Fever in the American Southwest
In the dry regions of California and Arizona, what worries residents every late summer and autumn is not the flu but a local fungal disease known as Valley fever, caused by Coccidioides. Strong winds lift the dry soil, and hidden fungal spores spread through the air. Once inhaled, symptoms like coughing, fever, or even pneumonia may appear within weeks.

The name is straightforward—it comes from the San Joaquin Valley, one of the earliest and most typical epidemic areas. For locals, “Valley fever” is not an unfamiliar medical term but a real and frequent concern.
Statistics highlight the scale: in 2024, California reported nearly 12,500 cases. In just the first half of 2025, Kern County alone recorded 1,945 cases, showing an upward trend. Each year, tens of thousands are infected. While most cases are mild or asymptomatic, about 1% of patients develop severe complications, with the infection spreading to the central nervous system or bones, leading to chronic or even fatal outcomes.
Cave Disease in River Valleys and Caves
Further east, in the Mississippi and Ohio River valleys, another endemic fungal disease appears: Histoplasmosis, often called Cave disease. This is not just a textbook name but directly linked to cave exploration and demolition work. Bat and bird droppings contaminate the soil, and when disturbed, fungal spores become airborne and can be inhaled.

According to CDC data, from 2019 to 2021 the United States reported 3,595 cases of histoplasmosis, with 1,459 cases in 2021 alone. While these numbers may only represent part of the true burden, they show that the disease is widespread. Most infections are mild or even without symptoms. However, for those with weakened immunity, the infection can spread to the liver, spleen, bone marrow, or central nervous system, sometimes becoming life-threatening.
Rose Gardener’s Disease in the Garden
Some fungal diseases stand in sharp contrast to the beauty of nature. Sporotrichosis, caused by Sporothrix schenckii, is nicknamed Rose gardener’s disease among horticultural workers. A prick from a rose thorn can allow the fungus to enter the skin and cause a slow, chronic infection under the tissue.

The name may sound poetic, but for those who love gardening, it is a real risk. In fact, sporadic cases have also been reported in Brazil, Mexico, and southern China, making this fungal “map” more vivid and more alarming.
The “Black Fungus” Crisis in Asia
In India, this warning became a shocking reality. During the COVID-19 pandemic, mucormycosis, a fungal disease long present in the environment, suddenly surged. Because infected tissue turned black, the media named it Black fungus.

By June 2021, India had recorded more than 40,800 confirmed cases and 3,129 deaths (BMC Infectious Diseases). At the peak, some hospitals admitted dozens of new patients every day. This outbreak was not caused by the sudden appearance of the fungus, but by a combination of factors: many COVID-19 patients with weakened immune systems, high prevalence of diabetes, and widespread use of corticosteroid drugs.
Mucormycosis has a very high fatality rate and progresses rapidly. Without prompt treatment, it can invade the eyes and brain within days, leading to blindness or death. For COVID-19 patients, “Black fungus” became a second deadly shadow. Although the name carries fear, it also made the public realize for the first time that fungi are not always harmless—they can claim tens of thousands of lives under the right conditions.
Africa’s Footprints: African Histoplasmosis and Madura Foot
In West Africa, African histoplasmosis (Histoplasma duboisii) is less well known internationally, but it commonly affects the skin and bones, posing a real health challenge in the region. Although large-scale statistics are lacking, it remains an endemic reality.
In Madagascar and other parts of Africa, another striking disease occurs: Madura foot (also called Mycetoma). This chronic infection begins when fungi enter through cracks in the skin, usually in people who work barefoot in the fields. The result is massive swelling and deformity of the foot, severely affecting the lives of farmers and herders.

A Data-Driven Warning for Everyday Life
Looking at this “global fungal disease map,” we see that hotspots are not far away: valleys, caves, and gardens in the United States, the pandemic-hit zones of India, and rural communities in Africa all hide fungal risks. These diseases may not spread like influenza, but they target specific climates, environments, and human behaviors to create localized hotspots.


One breath of dusty air, one prick from a plant thorn, or one episode of lowered immunity may open the door to infection. Fungi are not just hiding in corners of the home or on spoiled food—they are deeply rooted in human environments and everyday practices.
Understanding this map is more important than simply fearing fungi, because it reminds us that knowledge is the best protection. On your next trip or outdoor adventure, you may well be standing on one of the “hotspots” of this fungal map.
References
- CDC – Valley Fever (Coccidioidomycosis)
- CDC – Histoplasmosis
- CDC – Sporotrichosis
- CDC – Mucormycosis
- CDC – Mycetoma
- WHO – Neglected Tropical Diseases: Mycetoma
- African Histoplasmosis – PubMed
- Coccidioides – Wikipedia
- Histoplasmosis – Wikipedia
- Sporotrichosis – Wikipedia
- Mucormycosis – Wikipedia
- Mycetoma – Wikipedia
- GAFFI – Burden of Disease Maps
- LIFE Worldwide – Endemic Mycoses
Key Takeaways
- Endemic fungal diseases (Valley Fever, Histoplasmosis, Blastomycosis, Paracoccidioidomycosis, Cryptococcosis) occur in distinct geographic ‘hotspots’ where specific environmental fungi naturally exist in soil.
- Many people living within endemic areas have no knowledge of local fungal disease risk, leading to delayed diagnosis when respiratory symptoms are misattributed to bacterial pneumonia or tuberculosis.
- Climate change is actively expanding the geographic range of several endemic fungi: Coccidioides (Valley Fever) has been confirmed in previously non-endemic regions of the Pacific Northwest and Canada.
- An estimated 90% of fungal infections in endemic areas go undiagnosed or are misdiagnosed—patients may receive multiple courses of antibiotics before fungal disease is considered.
- Global travel increases the importance of endemic fungal disease awareness for all physicians: a traveller returning from an endemic area with respiratory symptoms may develop disease months after leaving.
Frequently Asked Questions
What are endemic fungal diseases and where do they occur?
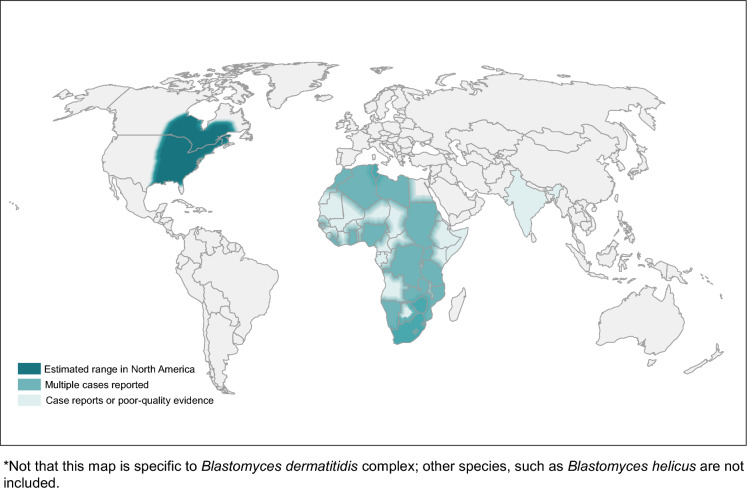
Endemic fungal diseases are infections caused by environmental fungi found in specific geographic regions—in contrast to opportunistic fungi (like Candida and Aspergillus) that infect susceptible hosts globally. The major endemic mycoses and their geographic distributions include: Coccidioidomycosis (Valley Fever, caused by Coccidioides immitis and C. posadasii)—endemic in arid areas of the US Southwest (California’s San Joaquin Valley, Arizona, New Mexico), Mexico, and parts of Central and South America; Histoplasmosis (caused by Histoplasma capsulatum)—Ohio and Mississippi River valleys in the US, Central and South America, sub-Saharan Africa; Blastomycosis (caused by Blastomyces dermatitidis)—Great Lakes region and Mississippi/Ohio River valleys; and Paracoccidioidomycosis (caused by Paracoccidioides brasiliensis)—Latin America, predominantly Brazil.
How do you contract an endemic fungal infection?
Most endemic fungal infections are acquired by inhaling spores (conidia) from environmental soil or decaying organic material in endemic areas. Specific risk activities include: construction, archaeological excavation, and soil disturbance in endemic areas (which releases spores into the air); military training exercises in arid desert regions; outdoor recreational activities including hiking, camping, and off-road driving that disturb soil; storm and dust events in arid regions (Coachella Valley dust storms have caused Valley Fever clusters); and occupational exposure in agriculture, landscaping, and wildlife management in endemic areas. Most healthy individuals who inhale spores experience mild or asymptomatic disease; severe infection primarily occurs in immunocompromised individuals, though severe Valley Fever can affect healthy people.
Why are endemic fungal infections so frequently misdiagnosed?
Endemic fungal infections mimic common bacterial respiratory infections clinically (fever, cough, chest pain, fatigue) and radiologically (pulmonary infiltrates, nodules, or consolidation that can look identical to bacterial pneumonia or lung cancer on chest X-ray). Most primary care providers and emergency physicians outside endemic areas have limited experience with these diseases. Standard bacterial cultures and viral tests are negative, but fungal testing is not routinely ordered unless the clinician specifically considers the diagnosis. Geographic residence history may not be taken, or patients may not realise that travel to an endemic area weeks or months earlier is relevant. Median time from symptom onset to diagnosis for Valley Fever is 22 days, during which patients typically receive multiple antibiotic courses without improvement.
Can you be in an endemic area and never get infected?
Yes—most people in endemic areas who encounter these fungi never develop clinical disease. For example, approximately 60–80% of long-term residents in Valley Fever-endemic areas of the US Southwest have positive skin tests indicating prior exposure, but the majority experienced only subclinical illness or mild self-limiting respiratory symptoms they attributed to a ‘cold’ or ‘flu.’ The immune system effectively contains these infections in healthy individuals through innate and acquired immune responses. Factors that increase the risk of severe disseminated disease include: HIV infection (CD4 <250); solid organ transplantation and immunosuppressive therapy; haematological malignancies; high-dose corticosteroid therapy; TNF-alpha inhibitors (used for rheumatoid arthritis); pregnancy; and in some studies, African American and Filipino ancestry for Valley Fever.
What should I do if I visit a Valley Fever or Histoplasmosis endemic area?
Most visitors to endemic areas do not develop significant disease and no specific preventive measures are fully proven effective. However, risk-reduction strategies include: avoiding activities that disturb soil (digging, construction) during your visit if you are immunocompromised; staying indoors during dust storms in arid regions; using N95 respirators if you must work in dusty conditions; not disturbing bird or bat roost sites (high-risk for Histoplasma from droppings); and informing your doctor of travel history if you develop respiratory symptoms within 1–3 months of the visit. If you have a weakened immune system, discuss fungal disease risk with your doctor before travelling to endemic areas—antifungal prophylaxis may be recommended for high-risk individuals visiting high-incidence areas.







