
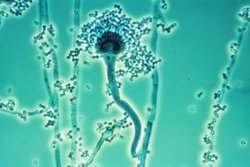
For decades, fungi have been quietly evolving. Now, a groundbreaking study from the Netherlands reveals the alarming pace at which some molds are developing resistance to our most trusted antifungal drugs. The spotlight is on Aspergillus fumigatus, a common airborne fungus that can cause deadly infections in people with weakened immune systems. And the implications stretch from the soil of industrial farms to the corridors of modern hospitals.
A Timeline of Trouble
Researchers from Radboud University Medical Center and the Dutch National Institute for Public Health and the Environment (RIVM) examined over 12,000 isolates of A. fumigatus collected from 1994 to 2023. In the 1990s, antifungal resistance in these samples was virtually nonexistent. But by 2023, nearly 17% showed genetic mutations that make them resistant to azoles, a class of antifungal compounds critical in both agriculture and medicine.

This is more than just a local issue. These resistant strains have been detected across continents—from Europe and Asia to South America and the U.S. Their spread is invisible but dangerous, driven by wind, travel, and even international trade. The global rise in fungal resistance is now undeniable.
From Crop Fields to Clinics
The culprit behind this resistance surge? Our own farming practices.
Azole fungicides are widely used in agriculture to protect crops like grains, vegetables, and flowers from fungal disease. These chemicals are molecular cousins to the azole drugs used in hospitals to treat patients. When A. fumigatus is exposed to these compounds in compost piles, crop residue, or soil, it evolves. Mutated strains thrive, survive, and eventually float through the air, landing in human lungs.

This agricultural-medical crossover means we’re unintentionally engineering drug-resistant pathogens in the wild, only to fight them again in ICUs.
The Medical Fallout
For patients with weakened immune systems—including those undergoing chemotherapy, recovering from organ transplants, or managing autoimmune diseases—these resistant fungal strains pose a serious threat. Treatment becomes more complex, outcomes more uncertain.
Many patients host multiple fungal strains simultaneously. This creates a Darwinian battlefield within the body, where resistant strains can quickly dominate if first-line drugs fail. Clinicians now need rapid diagnostics, better fungal typing, and alternative treatments to keep up.
Why Antifungal Innovation Lags
Developing new antifungal drugs is a scientific challenge. Fungi, like humans, are eukaryotes—they share similar cellular machinery. That makes it harder to target them without also harming human cells. As a result, antifungal innovation has lagged far behind antibacterial drug development.
Emerging technologies, like 18F-FDS PET imaging, may help detect mold infections earlier. But effective treatment still depends on timely diagnosis, resistance testing, and access to drugs that work.

A Call to Action
The Dutch study serves as both a warning and a roadmap. Experts are calling for:
- Global surveillance of environmental and clinical fungal resistance
- Stricter regulations on agricultural fungicide use
- Investment in new antifungal drug classes
- Improved diagnostic technologies to detect resistance in real time
There’s also a growing call for One Health approaches—coordinated strategies that connect human, animal, and environmental health. Because when the air we breathe carries drug-resistant spores, no sector can afford to work in isolation.

The health of people is closely connected to the health of animals and our shared environment.
The Clock Is Ticking
What began as a slow biological shift has now accelerated into a global public health issue. Resistant fungi are spreading faster than our ability to treat them. Without action, more patients will face failed therapies, longer hospital stays, and higher mortality rates.
But the path forward is clear. We need smarter surveillance, better stewardship, and faster innovation. The next generation of antifungal tools must be rooted not just in labs, but in the awareness that what we do to the land inevitably finds its way into our bodies.
The enemy is adapting. Our response must evolve even faster.
References
Key Takeaways
- Drug-resistant mold infections—particularly azole-resistant Aspergillus fumigatus and multi-drug-resistant Candida auris—are increasing globally, leaving some patients with no effective antifungal treatment options.
- Only three classes of antifungal drugs exist for systemic infections (azoles, echinocandins, and polyenes), compared to dozens of antibiotic classes for bacteria—reflecting decades of underinvestment in antifungal development.
- Resistance in Aspergillus fumigatus is driven not only by clinical antifungal use but by environmental exposure to agricultural triazole fungicides, with pan-azole-resistant strains detected in patients who have never received antifungal therapy.
- Two novel antifungal agents—ibrexafungerp (first-in-class triterpenoid) and olorofim (first-in-class dihydroorotate dehydrogenase inhibitor)—received regulatory approval in 2021–2022, beginning to address the sparse pipeline.
- Global antifungal stewardship programmes are being developed to preserve the effectiveness of existing antifungal drugs, analogous to antimicrobial stewardship programmes for antibiotics.
Frequently Asked Questions
Why are so few antifungal drug classes available compared to antibiotics?
The relative scarcity of antifungal drug classes reflects the fundamental challenge of fungal biology: fungi are eukaryotes (cells with nuclei, similar to human cells) rather than prokaryotes like bacteria. Most antibiotic mechanisms target structures unique to bacteria—cell wall synthesis using peptidoglycan (absent in humans), bacterial ribosomes (structurally different from human ribosomes), or specific bacterial metabolic pathways. Antifungal targets must be present in fungi but not human cells. The three established targets are ergosterol (fungal cell membrane sterol, different from human cholesterol—targeted by azoles and polyenes), fungal cell wall beta-glucan synthesis (targeted by echinocandins), and fungal-specific nucleic acid synthesis (targeted by flucytosine). Finding additional targets unique to fungi that are not essential in humans has proved extremely difficult.
What is the TR34/L98H mutation and why is it important for understanding azole resistance?
TR34/L98H is the most clinically significant azole resistance mutation in Aspergillus fumigatus globally. It consists of a 34-base-pair tandem repeat (TR34) in the promoter region of the CYP51A gene (which encodes the azole drug target) combined with a leucine-to-histidine substitution at codon 98 (L98H). The TR34 insertion causes overexpression of the CYP51A enzyme (more drug target—more drug needed to block it), while L98H alters the enzyme’s shape to reduce azole binding affinity. Together, these cause pan-azole resistance: strains with this mutation are resistant to all currently approved azole antifungals simultaneously. Critically, the TR34/L98H genotype appears to have arisen primarily in environmental Aspergillus populations exposed to agricultural triazole fungicides, not in clinical settings.
What are the newest antifungal drugs and how do they work?
Several novel antifungal agents reached clinical approval or advanced trials since 2020. Ibrexafungerp (Brexafemme, US approval 2021) is the first triterpenoid antifungal—it inhibits beta-1,3-glucan synthase (the same enzyme as echinocandins) but binds at a different site, maintaining activity against some echinocandin-resistant strains. Olorofim (2023 FDA breakthrough therapy designation; approved in some markets) is the first dihydroorotate dehydrogenase (DHODH) inhibitor antifungal, blocking a step in pyrimidine biosynthesis in fungi but not mammals; it is particularly active against Aspergillus and some Mucorales. Fosmanogepix (APX001A prodrug) is a novel Gwt1 inhibitor blocking fungal cell wall glycosylphosphatidylinositol (GPI) anchoring, active against Candida auris. These represent the first genuinely new antifungal mechanisms in two decades.
What is antifungal stewardship and how does it differ from antibiotic stewardship?
Antifungal stewardship programmes (ASPs) apply the same principles as antimicrobial stewardship to antifungal drug use: optimising the selection, dose, route, and duration of antifungal treatment to minimise resistance development and drug toxicity while maintaining clinical efficacy. The principles are similar to antibiotic stewardship (appropriate indication, de-escalation when possible, shortest effective duration) but face specific challenges: the diagnostic delay that leads to prolonged empirical therapy; the need to use broad-spectrum antifungals empirically while awaiting diagnostic results; and the complex patient populations (severely immunocompromised) where under-treatment mortality is high. Antifungal stewardship is less developed than antibiotic stewardship globally, partly due to the smaller number of antifungal experts and the less prominent public health recognition of antifungal resistance.
How can patients avoid contributing to antifungal resistance?
Patients can take several steps to avoid contributing to antifungal resistance. Follow prescribing guidance: take the complete course of antifungal treatment as prescribed, even if symptoms resolve; do not save antifungal medications for future use; do not share antifungal prescriptions. Avoid non-prescription azole antifungals except where specifically indicated (over-the-counter azole creams for skin fungal infections should be used only for confirmed fungal conditions, not prophylactically). Be cautious with dietary supplement antifungals (essential oils, herbs claimed to have antifungal properties) as these may have subtherapeutic concentrations that expose organisms to insufficient drug pressure. Ask prescribers about antifungal stewardship: in hospitals, ask about diagnostic testing to guide therapy and about de-escalation from broad to narrow spectrum antifungals when possible.







